


How to Recover from Shoulder Surgery: Chapter 2: A User’s Guide to the Shoulder

The shoulder is easily the most amazing joint in the human body. If you don’t believe me, watch international level gymnastics sometime and take notice of the incredible things that athletes do with their shoulders.
The shoulder has the largest range of movement of any joint in the body, and yet with the right training and fitness people can walk on their hands or carry out amazing manoeuvres on Roman rings at gymnastic competitions.
Analysing these abilities of the shoulder, we can see that the shoulder has mobility, strength and stability. These three are often seen as being mutually exclusive, but the shoulder manages all three in its optimum state.
So how does the shoulder girdle manage this? Because it comprises a complex of joints which are stabilised by a complex arrangement of muscles and ligaments:
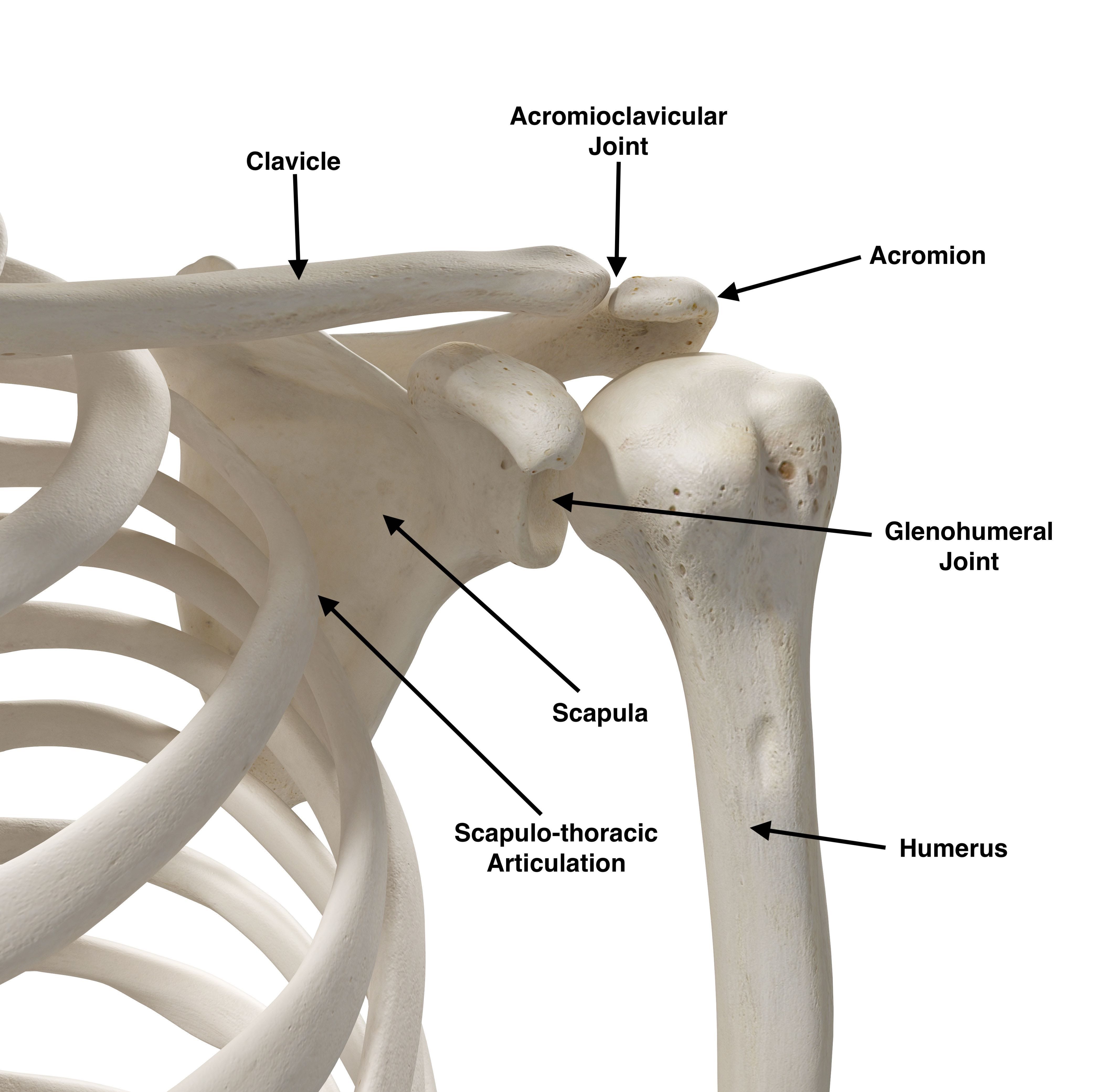
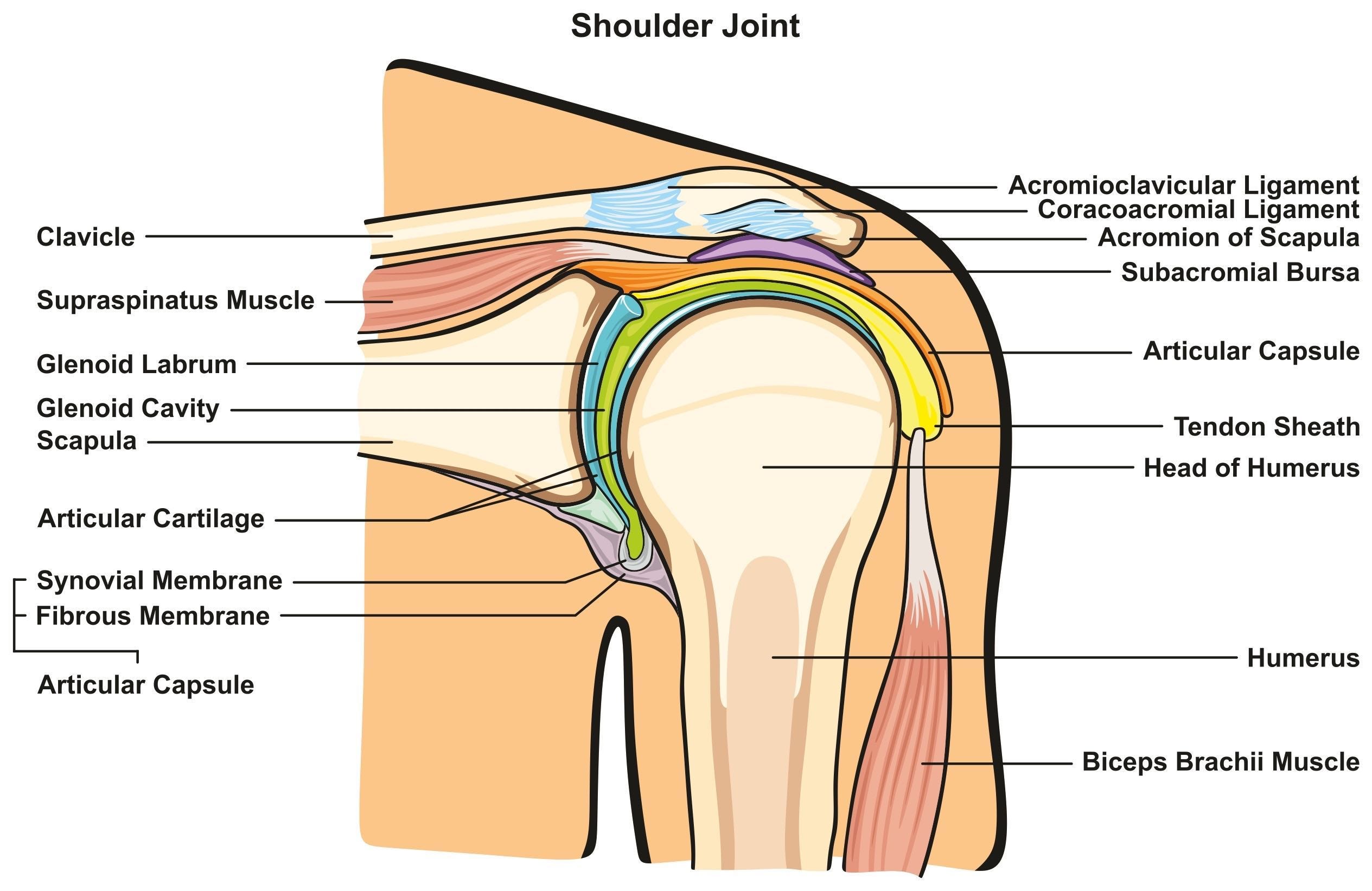
◆ The glenohumeral joint (GHJ) is the “ball and socket” joint between the humerus (upper arm bone) and the scapula (shoulder blade). The socket is deepened by a ring of cartilage—the glenoid labrum. The glenoid labrum provides better stability.
◆ The acromioclavicular joint (ACJ) is the joint between the acromion (part of the scapula) and the clavicle (collar bone).
◆ The scapulothoracic articulation is not actually a joint but an area where the scapula moves across the ribs under the control of several muscles.
These joints are moved by and stabilised by a range of muscles. The most important group of muscles for the GHJ is the Rotator Cuff—the Supraspinatus, Infraspinatus, Subscapularis and Teres Minor muscles. These muscles attach the scapula to the head of the humerus and stabilise the GHJ. Their tendons form a cuff around the head of the humerus, providing both movement and stability.
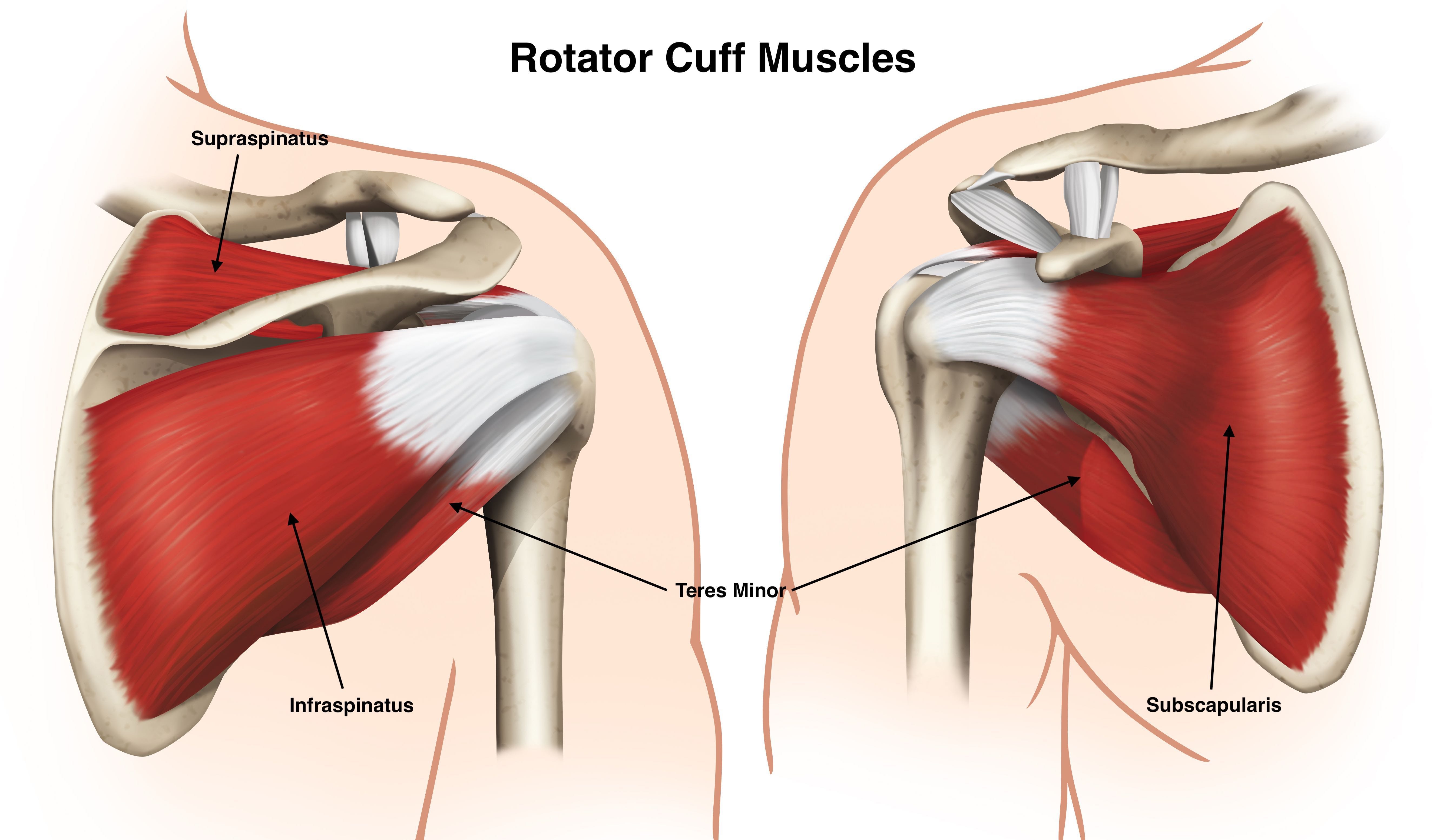
Without a functioning rotator cuff, we are actually unable to raise our arm past horizontal. At the very least we experience shoulder pain on overhead activities, as the humeral head can rise compressing the subacromial/subdeltoid bursa. Damage to the rotator cuff is one of the most common reasons for shoulder surgery.
The GHJ is surrounded by a joint capsule, a sleeve of ligamentous type tissue strengthened by several ligaments. A potential complication of shoulder surgery is “frozen shoulder”, where the capsule becomes inflamed and ultimately thickened and tight. This can cause restricted and painful movement and delayed recovery.
So in summary the glenohumeral joint:
◆ is a large ball sitting in a small shallow socket,
◆ is held together by a loose joint capsule (to allow a large range of movement),
◆ has a capsule strengthened by several ligaments,
◆ is stabilised by the rotator cuff group of muscles and their tendons, and
◆ is moved by many muscles travelling between the spine, thorax, scapula and upper arm.
In this way the shoulder meets our requirements of mobility, stability and strength. It does however leave the shoulder susceptible to any injury or degenerative changes of these structures.
Although a rehabilitation exercise program can achieve a lot, there will be times where surgical help is required.
If you want to see how all these structures move together, I suggest other shoulder anatomy resources at: